Mental Health Printable Release Of Information Form
Free 9 Sample Release Of Information Forms In Ms Word Pdf

Editable Forms For Release Of Mental Health Information Fill

Printable Health Information Release Authorization Form
Health information have already taken action because of my earlier authorization.
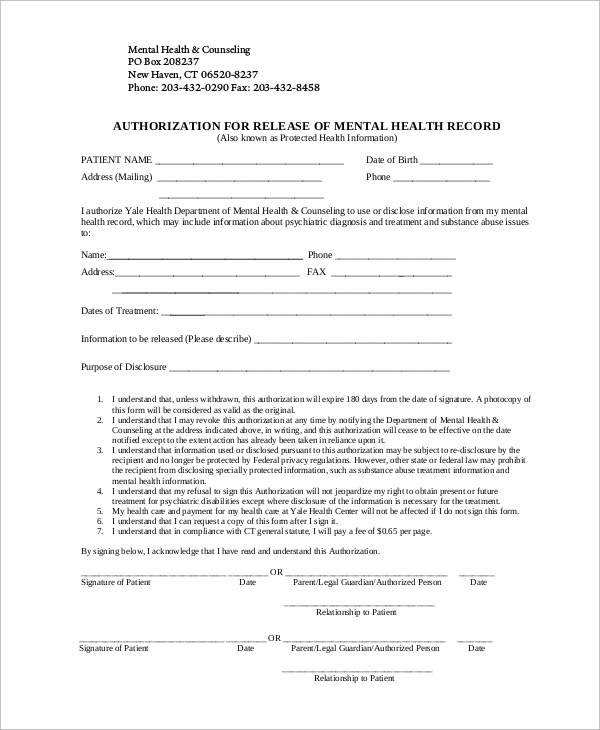
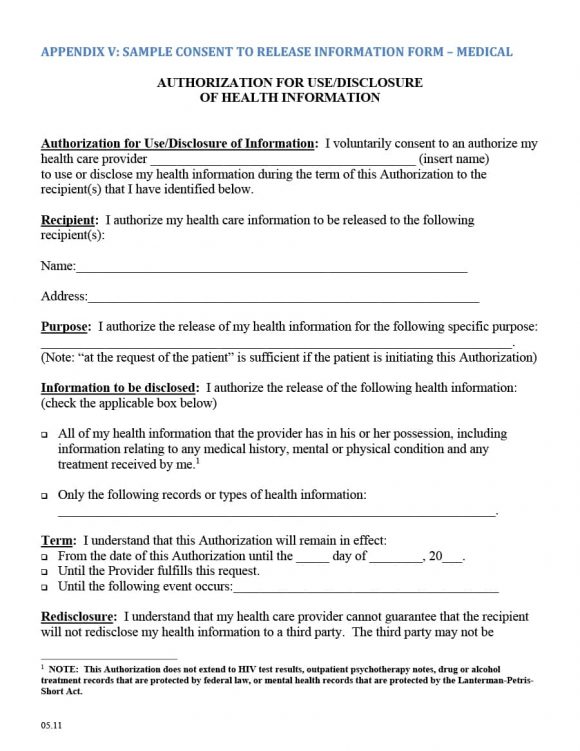
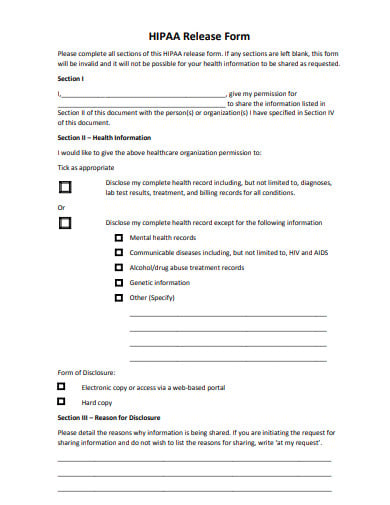
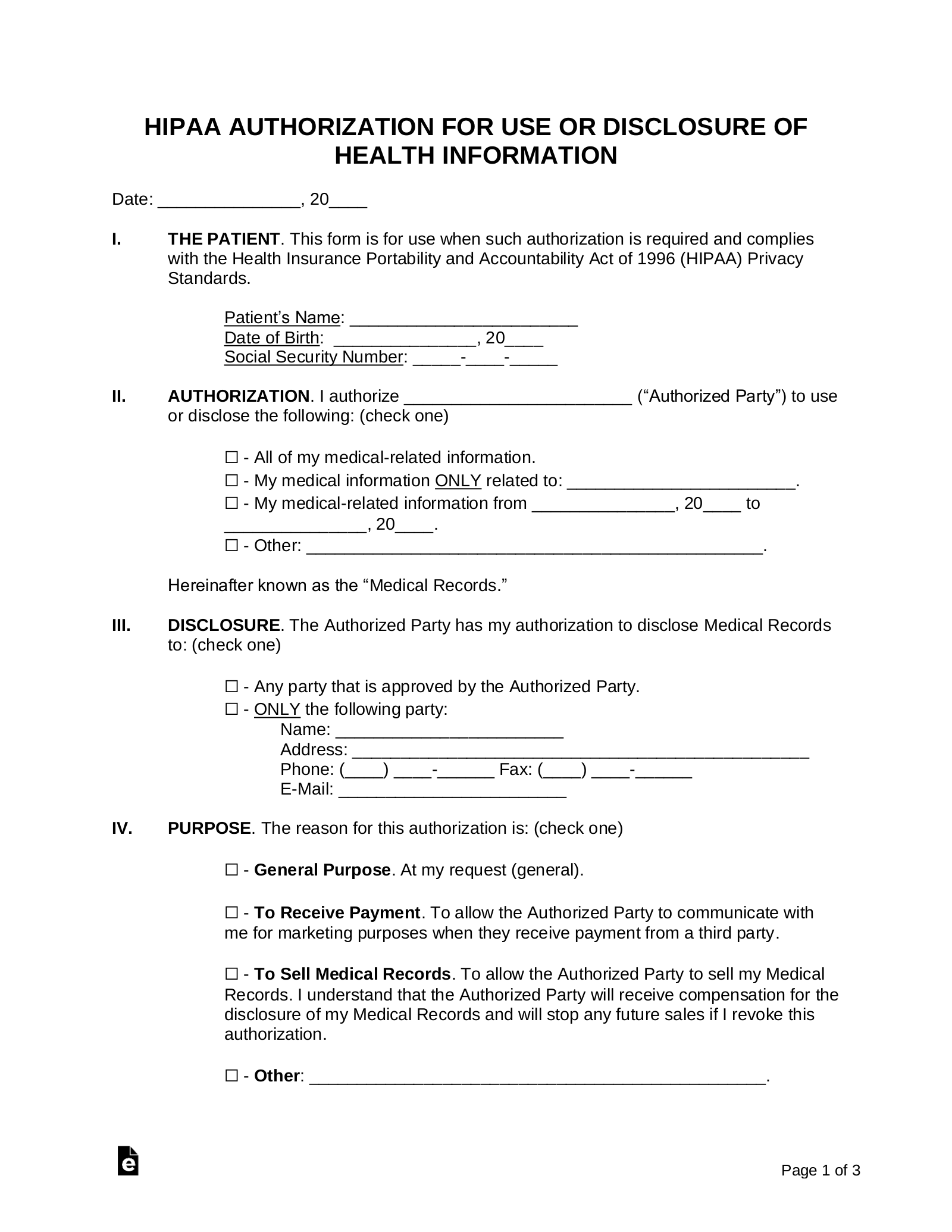
Mental health printable release of information form. This form will be considered as valid as the original. Mental health certification forms. Authorization for release of health information pursuant to hippa. The release of information form is used when you are going to submit a written request to a body an organization your insurance provider your work organization or some government body to release some information.
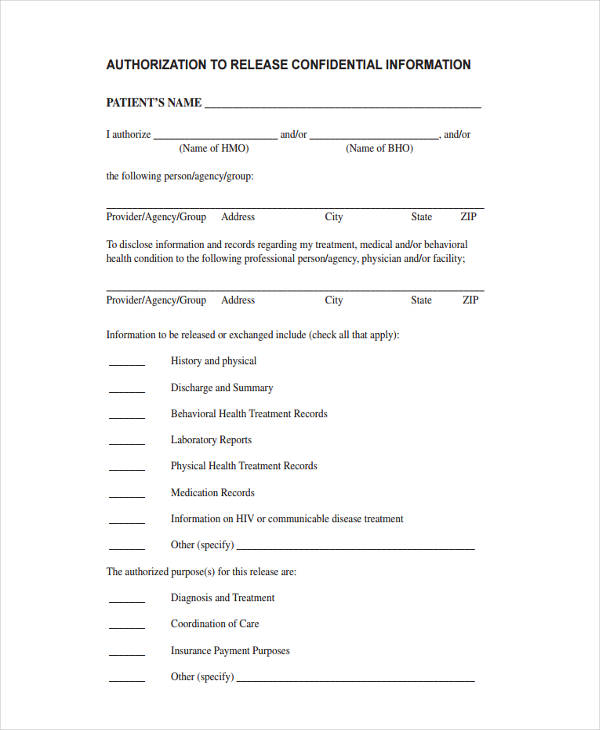
Authorization for release of mental health record. Fillable and printable release of information form 2020. I understand that i may revoke this authorization at any time by notifying the department of mental health. For disclosure of mental health treatment information i insert name of patientclient whose date of birth is authorize insert name of mental health counseling organization to disclose to andor obtain from.
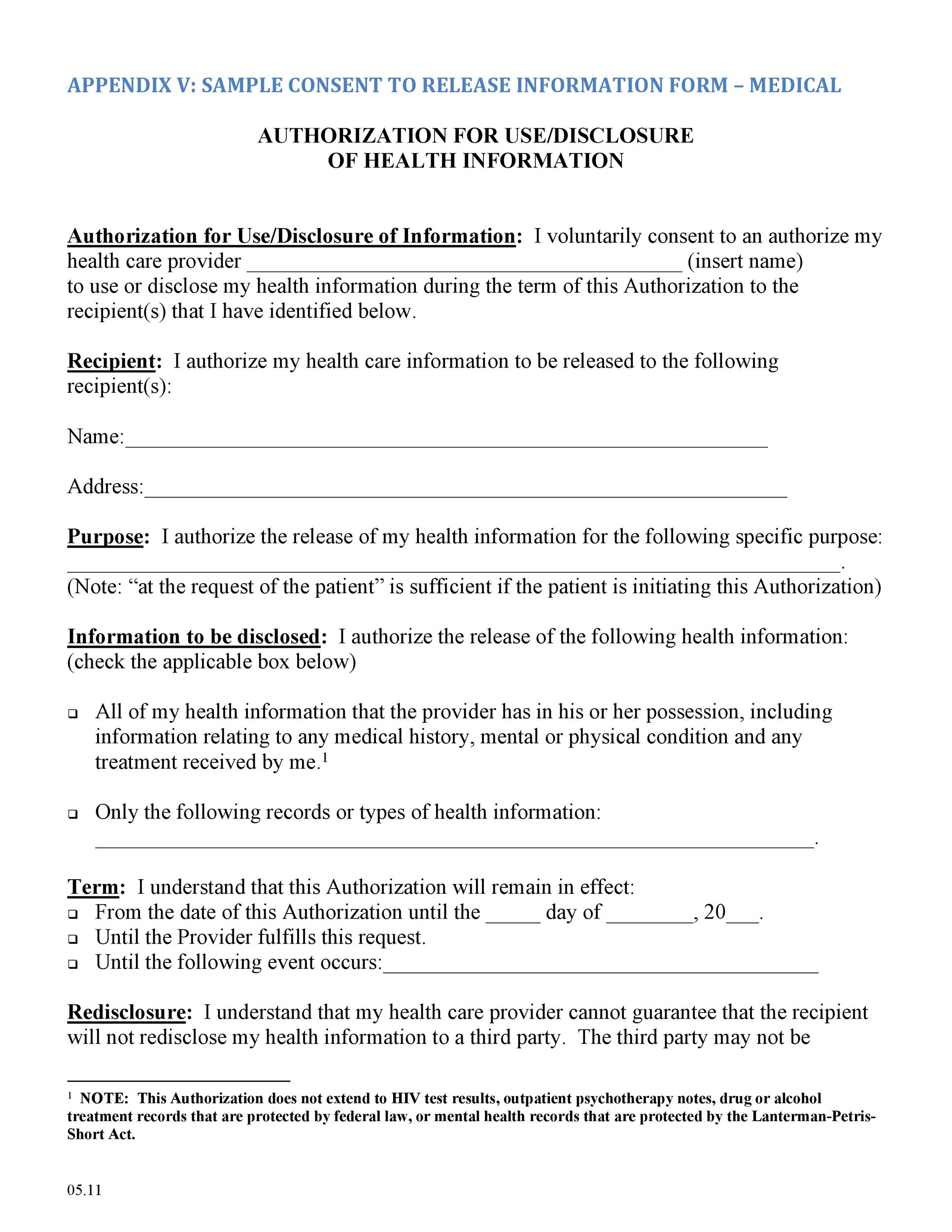
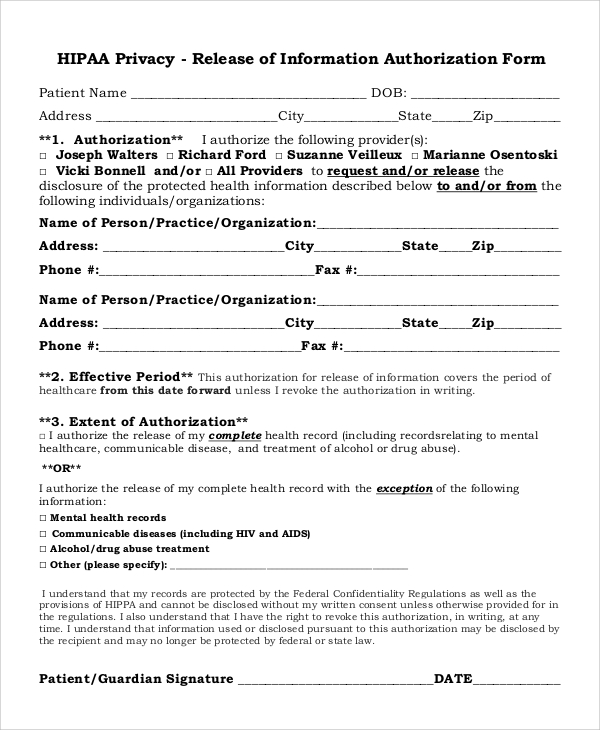
9 sample release of information forms. I understand that state law requires each clients consent for the release of confidential information related to mental health or developmental disability. Home release form. The medical record information release hipaa also known as the health insurance portability and accountability act is included in each persons medical file.
Mental health history tothe extent that the latter information relates to the ability of. Dhcs 1800 mh 300. However this form does not require health care providers to release health information. The release of lnfomriation form allows.
Compensation commission authorization for release of medical. This form may be used in place of doh2557 and has been approved by the nys office of mental health and nys office of alcoholism and substance abuse services to permit release of health information. I do not have to sign this authorization and that my refusal to sign will not affect my abilities to obtain treatment from the new york state office of mental health nor will it affect my eligibility for benefits. With this understanding i hereby waive any right to confidentiality arising under state law and authorize the release of records of information but only the extent specified below.
I understand that my refusal to sign this authorization will not jeopardize my right to. Electroconvulsive treatment ect informed consent form spanish dhcs 1801 mh 302. Application for assessment evaluation and crisis intervention or placement for evaluation and treatment. Sources of a information.
Electroconvulsive treatment ect informed consent form. A copy of the bar application release of information form.

Release Of Medical Records Form Medical Records Medical

Free 13 Sample Release Of Information Forms In Pdf Ms Word

Fillable Online Release Of Information Form Pine Rest Fax Email
12 Hipaa Release Form Templates In Pdf Doc Free Premium
30 Medical Release Form Templates ᐅ Template Lab

Mental Health Release Form Fill Out And Sign Printable Pdf
Free Medical Records Release Authorization Form Hipaa Pdf
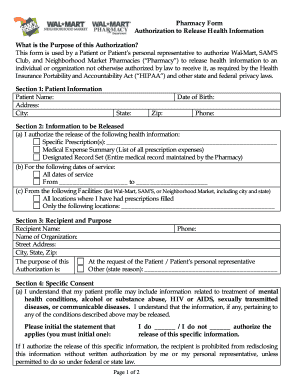
Walmart Authorization To Release Form Fill Out And Sign
Free 8 Sample Hipaa Release Forms In Pdf Ms Word
Free 17 General Release Of Information Forms In Pdf Ms Word

Work Release Form From Hospital Lovely Awesome Work Release Form

40 Medical Records Release Form Release Of Information
Authorization To Release Healthcare Information Form Printable
12 Hipaa Release Form Templates In Pdf Doc Free Premium
Form Hipaa F 8 Download Printable Pdf Or Fill Online Authorization
Authorization For Release Of Health Information Pursuant To Hippa

Pin On Food

General Release Of Information Form Template
